It’s double time! For those bandies and musicians or Tae-bo pros out there, you know this means it’s time to pick up the pace.

During the 2nd trimester, from weeks 15 to 20, babies double in size. So, you can imagine that the nutrient needs of both mom and babies alsoescalate. There are a variety of methods to determine how many calories are ideal during pregnancy. There are estimated energy requirement equations, some just say 300 extra calories and 30 extra grams of protein per day, and others encourage moms to add 500 calories per fetus and 25g protein. I, personally, think it is best to consume the amount of calories that promotes the ideal weight gain per week. For a mom of high order multiples it is 2.0-2.5 lbs. per week.
I was able to gain this at 3,000 Calories per day during the first trimester. This was a true blessing because with the nausea there was no way I was going to get to the original 5,000-calorie estimation. During weeks 13 to present, I have watched this weight gain slow-down, so I know it’s time to bump up the kCals. I really was quite surprised that there were not any meal plan examples- that I could find anyway- on the Internet. My best resource was in Dr. Barbara Luke’s book, “When you’re expecting twins, triplets, or quads.” This is where I derived the information regarding calorie and food group goals. Since there seems to be a gaping whole on the World Wide Web, I thought I’d go ahead and fill it.
Below you will find recommendations for calories, macronutrients (carbs, protein and fat) and suggested food group goals during pregnancy. While this information is targeted at high order multiple pregnancies, it is of course applicable to any pregnancy.
Calories goals may vary from 3,000-5,000 Calories per day, and I recommend watching your average weight gain from week-to-week to be sure you are getting enough. The composition of these Calories is important and different than the recommendations for the average American. Typically, it is recommended to consume a daily diet composed of 50-55% calories from carbohydrate, 15-20% calories from protein and 25-30% calories from fat. However, during pregnancy with super twins it is recommended to consume 40% of calories from carbohydrate, 40% calories from fat and 20% calories from protein. The reduction in calories from carbohydrate, I presume is to decrease one’s risk of gestational diabetes, which is much higher in pregnancies with 3 or more. Per Dr. Luke, this breaks down to the following:
| Nutrients |
3,000
|
3,500
|
4,000
|
4,500
|
| Protein |
150g
|
176g
|
200g
|
225g
|
| Fat |
133g
|
155g
|
178g
|
200g
|
| Carbohydrate |
300g
|
350g
|
400g
|
450g
|
|
|
|
|
|
| Food Groups |
Servings per day
|
| Lean Protein |
4
|
5
|
5
|
6
|
| Dairy |
4
|
8
|
10
|
12
|
| Grains |
8
|
10
|
12
|
12
|
| Fat |
5
|
6
|
7
|
8
|
| Fruit |
7
|
7
|
8
|
8
|
| Vegetables |
4
|
4
|
5
|
6
|
This type of meal plan is quite different than my pre-pregnancy diet, so my typical pattern is a bit different. For example, prior to pregnancy I ate very little dairy and meat/poultry and the majority of my protein came from beans, peas, lentils, whole grains, and fish. It has been easiest for me, and my mild lactose intolerance, to add the lean meats versus 8-10 servings of dairy per day. Also, before pregnancy I ate a lot of veggies and not so many fruits, so I continue to consume only 2-3 fruits per day and 8-plus servings of vegetables.
As mentioned previously, I have been consuming 3,000-3,500 Calories per day so I decided to share a few meal plans, or as RD’s call them “Typical days” to help make these recommendations real. There are a few original high calorie, high protein recipes in the meal plans that I will add later. If you’re interested check back because I will be adding a recipe section to my blog. Also, I did not comment on the variety of supplements that I believe are a crucial safety net, so look out for that content coming soon!
Day 1
(3,065 Calories: 316g Carb, 92g Fat, 175g Protein)
Breakfast
- Breakfast Taco Dip
- ½ tsp Olive Oil
- 1 Organic Egg
- ½ Avocado
- 4oz 0% Plain Greek Yogurt
- Lentil Loaf (Recipe coming soon)
- 2 Hard Shell Tacos, broken into chips
- Up Your Mass™ Banana Smoothie (Recipe coming soon)
AM Snack
- Fruit and Yogurt Parfait with Granola
- ½ cup Fresh berries
- 1 cup Low-fat Vanilla yogurt
- ¼ cup Nutty Granola
Lunch
- Turkey and Avocado Sandwich
- 2 slices Homemade Whole Wheat Bread
- 3 oz Oven-roasted Turkey Breast*
- ½ Avocado
- 1 cup Fresh Spinach
- 2 Clementines
- ½ Cup Baby Carrots
PM Snack
- Oat and Nuts Cereal
- 1 ¼ C Oat Cereal
- 1 C Unsweetened, Organic Soy Milk
- ¼ C Roasted Pepitas
- ¼ C Slivered Almonds
Dinner
- Basil Mac & Cheese (Recipe coming soon)
- 12 medium shrimp, cooked
- 1 C Asparagus Spears
- Skinny Cow™ Ice Cream Sandwich
Evening snack
- PowerBar™ Harvest Peanut Butter Chocolate
Day 2
(2,993 Calories: 319g Carb, 94g Fat, 171g Protein)
Breakfast
- 4 Up Your Mass™ Banana Nut Pancakes (Recipe coming soon)
- 1 C Unsweetened, Organic Soy Milk
AM Snack
- Cinnamon Raisin Bagel with 1oz Cream Cheese
- 1 C 2% Milk
Lunch
- 1 Large Baked Potato with Lentil Loaf, melted Cheese stick and 2 Tbsp Salsa
- 1 C Asparagus spears
- 1 C Fresh Pineapple
Dinner
- ¾ C Cooked Quinoa with 1 tsp Olive oil
- 4oz Organic, Skinless Chicken Breast
- 1 C Steamed Zucchini Squash
- Skinny Cow™ Ice Cream Sandwich
Day 3
(3,710 Calories: 367g Carb, 154g Fat, 176g Protein)
Breakfast
- Stuffed Baked Potato
- 1 Large Baked Potato
- ½ tsp Olive Oil
- 1 organic Egg and 1 Egg white
- 1 Melted Cheese stick
- ¾ C Kidney Beans
- ¼ C Salsa
AM Snack
- ¼ C Dried Fruit
- ½ C Almonds and Pumpkin seeds, mixed
- 1 C Organic Skim Milk
Lunch
- ¾ C Pasta with ½ C Meat Tomato Sauce and ¼ C Melted Mozzarella Cheese
- 1 C Steamed Spinach
- 1 Banana
- 2 Tbsp Peanut Butter
PM snack
- 1 Whole Wheat Pita
- ½ C Original Hummus
Dinner
- 5 oz Salmon with ¼ C Avocado Salsa
- 1 C Wild and Brown Rice
- 1 C Steamed Broccoli
Evening Snack
- 1 ½ C Neapolitan Ice Cream**
* I try not to consume deli meat, so this was a baked turkey breast. I do reheat any lunch meat/protein that I bring as a food safety precaution.
** When you want to promote glycemic (blood sugar) control, eating sweets and desserts alone is a no-no. However, if the dessert is consumed within 1 hour of a meal or healthier snack, typically the blood sugar response is more favorable.
Written by: Cassie Vanderwall, MS RD CD CDE CPT

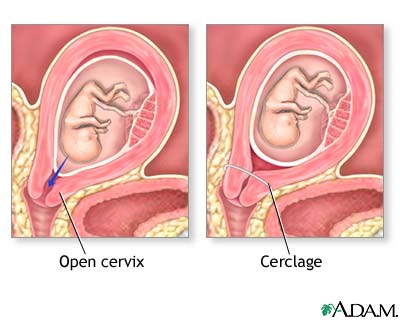
 Sir Clahj, is not a character from Medieval times, but it is rather how you pronounce the surgical procedure, cerclage, which is the “knight in shining armor” who has saved our pregnancy.
Sir Clahj, is not a character from Medieval times, but it is rather how you pronounce the surgical procedure, cerclage, which is the “knight in shining armor” who has saved our pregnancy.